

In the pharmacokineticsDiY part 1 the numerical approach of pharmacokinetic calculations was explained. Using relative simple formulas implemented in a spreadsheet the concentrations of a drug could be calculated following variable drug input protocols. The Eleveld model for propofol was used. This was not without a reason. Douglas Eleveld and co-authors analyzed the data from numerous other studies, collected in the open Target Controlled In fusion(TCI) initiative, to develop a pharmacokinetic and pharmacodynamic model for broad application in anaesthesia and sedation.
Their work is a milestone in the development of Pk/Pd models that will improve the clinical usability of Target Controlled Infusion systems and the understanding and interpretation of the observed effect related to these models. Until recently most of the implemented models in Target Controlled Infusion systems were limited in usability and hampered by unverified extrapolation of data from studies that were not intended to deliver robust, population models for TCI. So a model for an 'average' patient could be unreliable or even be proven wrong for a paediatric or obese patient. But appart from an elaborated relation with antropometric properties, age, weight etc, they also found a dependency of the pharmacokinetic model with the co-administration of opioids. The influence of an opioid on the pharmacokinetics of propofol has been studied before and one of the possible explanations is that the influence of opioids on the heart rate and thereby the cardiac output could change the clearance of propofol by decreasing the liver flow. Antropometric properties, age,weight,length, gender usually do not change during an application of TCI but whether or not, and the point in time an opioid is administerd may vary in clinical situations.
The influence of the opioid on the pharmacokinetics of propofol is a small example of the complexity of the anaesthetic state that is the resultant of anaesthetic drugs, surgical stimuli and responses of the patient who has its own internal regulation and homeostasis processes for the most part intact because the patient is alive. Observation as the titration paradox are in my opinion not surprising and only prove that we do not understand the full complexity of this state.
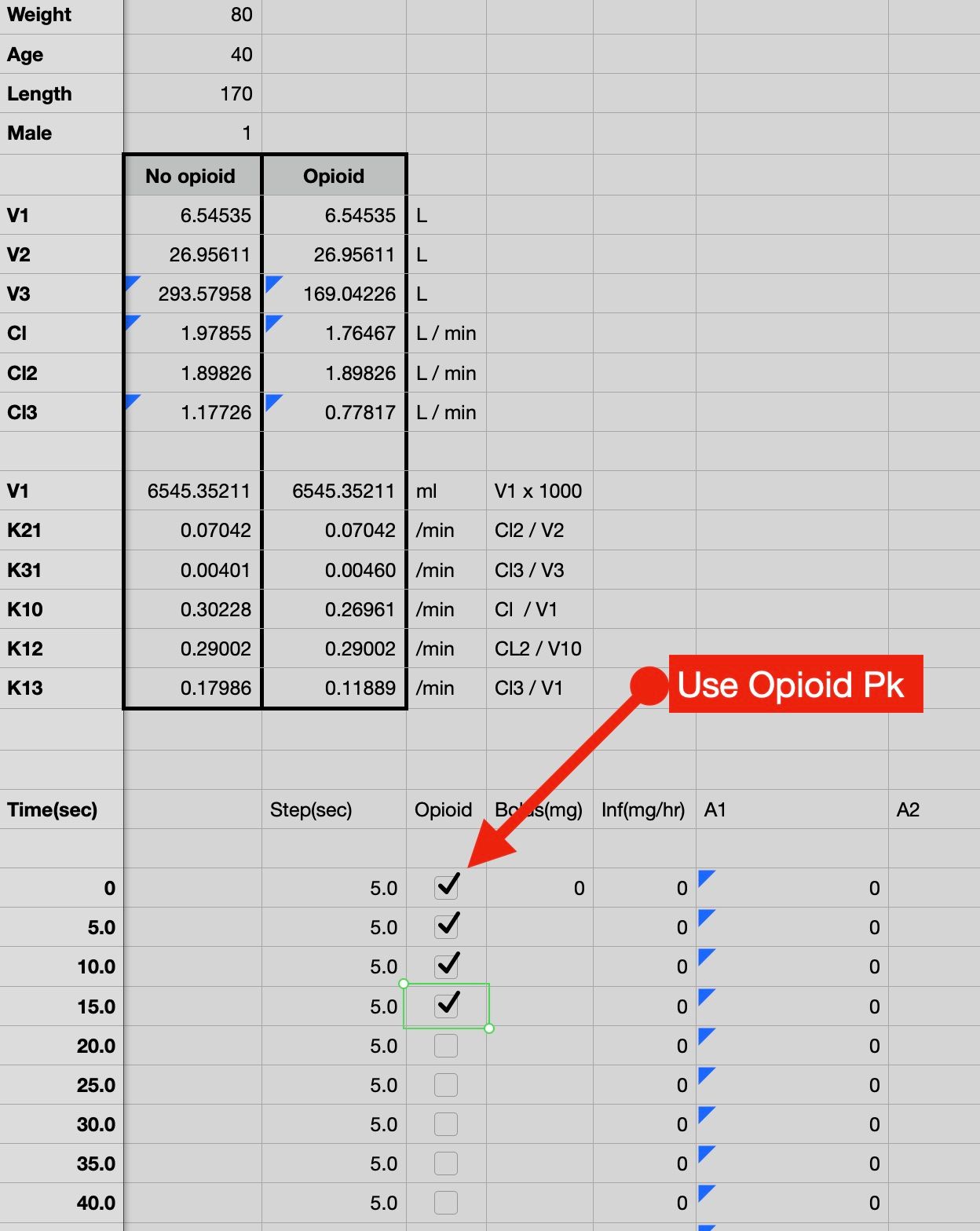
With the spreadsheet presented in this blog the effect of an opioid on the pharmacokinetics can be switched on or off. The effect on the pharmacokinetics of propofol is binary, it is present or it is not. So the amount of opioid does not influence the effect(at least not in the model). In part 1 it was shown that the time interval of 5 seconds was more than enough to deliver a highly accurate simulations in comparison with TivatrainerX that uses an analytical('exact') calculation. Again the results of the simulation are verified with the overlay approach as explained in part 1. If we look at the differences between the pharmacokinetic set with and without opioid we see that the clearance decreases together with the size of the 3th compartment. In timeconstants: k10,k31 and k13. Using the offset function in a spreadsheet the correct values are selected dependent on the tickbox (Numbers) or TRUE/FALSE (excel) value in the 'opioid' column[D].
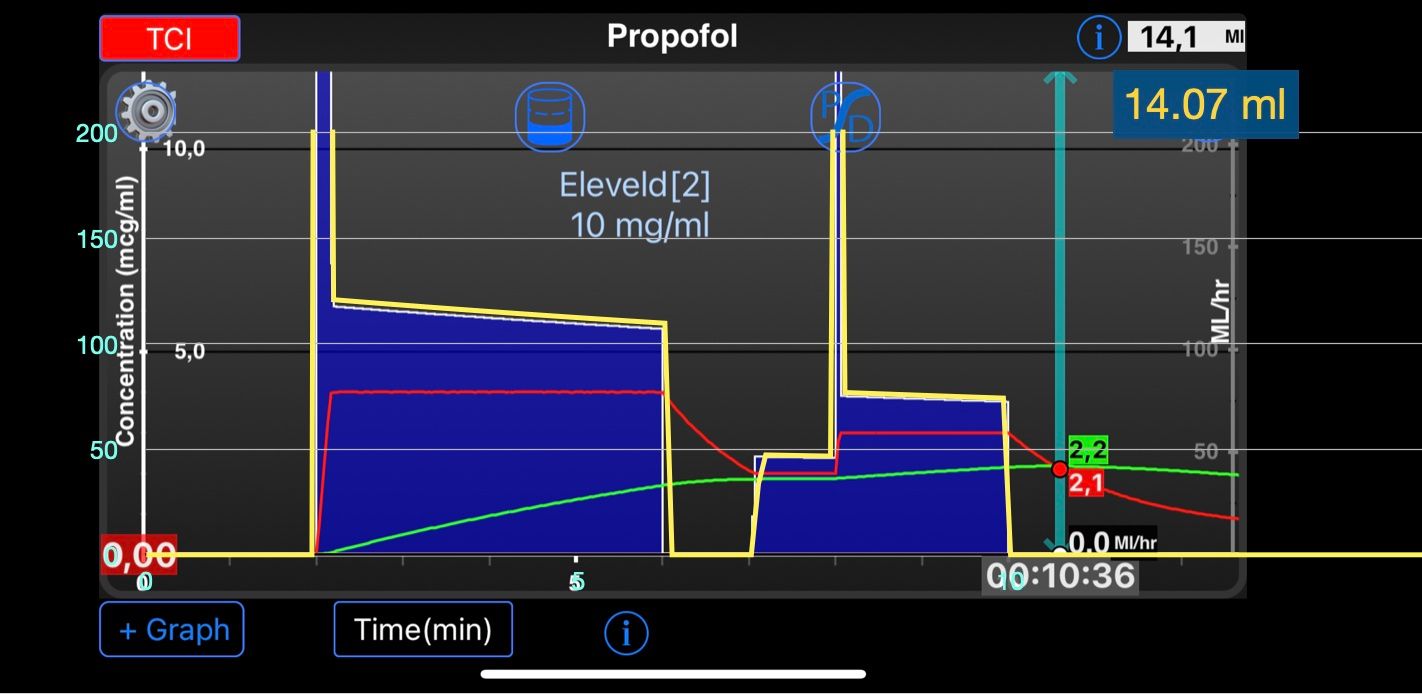
In order to simulate a real live scenario also a TCI simulation is added. This is done in the sheet called TCI. Calculation is based on the same principles of the Euler approximation for the Pk model: the infusion to achieve and maintain a specific concentration is a loading infusion amount: target * V1. Subtracted from this amount is the amount already present and subsequently in following steps drug is replaced that is lost from the central compartment with an equal amount by infusion. Negative drug input is impossible and there is a limitation of the maximum rate a pump can deliver(this can be adjusted).These constraints are implemented with simple If.. Else statements. If the input is negative it is zero, if the input is larger than the infusion pump can deliver then the input equals this maximum. The verification of the implemention of the pharmcokinetics with opioid has been done similar to the verification of the pharmacokinetics in part 1. For verification of the TCI sheet a target scheme was compared with TivatrainerX. Differences are neglectible and the total amount predicted by TivatrainerX: 14.1 ml was comparable to the total amount of the numerical appraoch: 14.07 ml.
It will be very unlikely that pumpmanufacturers will allow a possible change between the two Pk Eleveld models: with or without opioid, during a TCI application, but with the spreadsheet some different scenarios can be investigated:
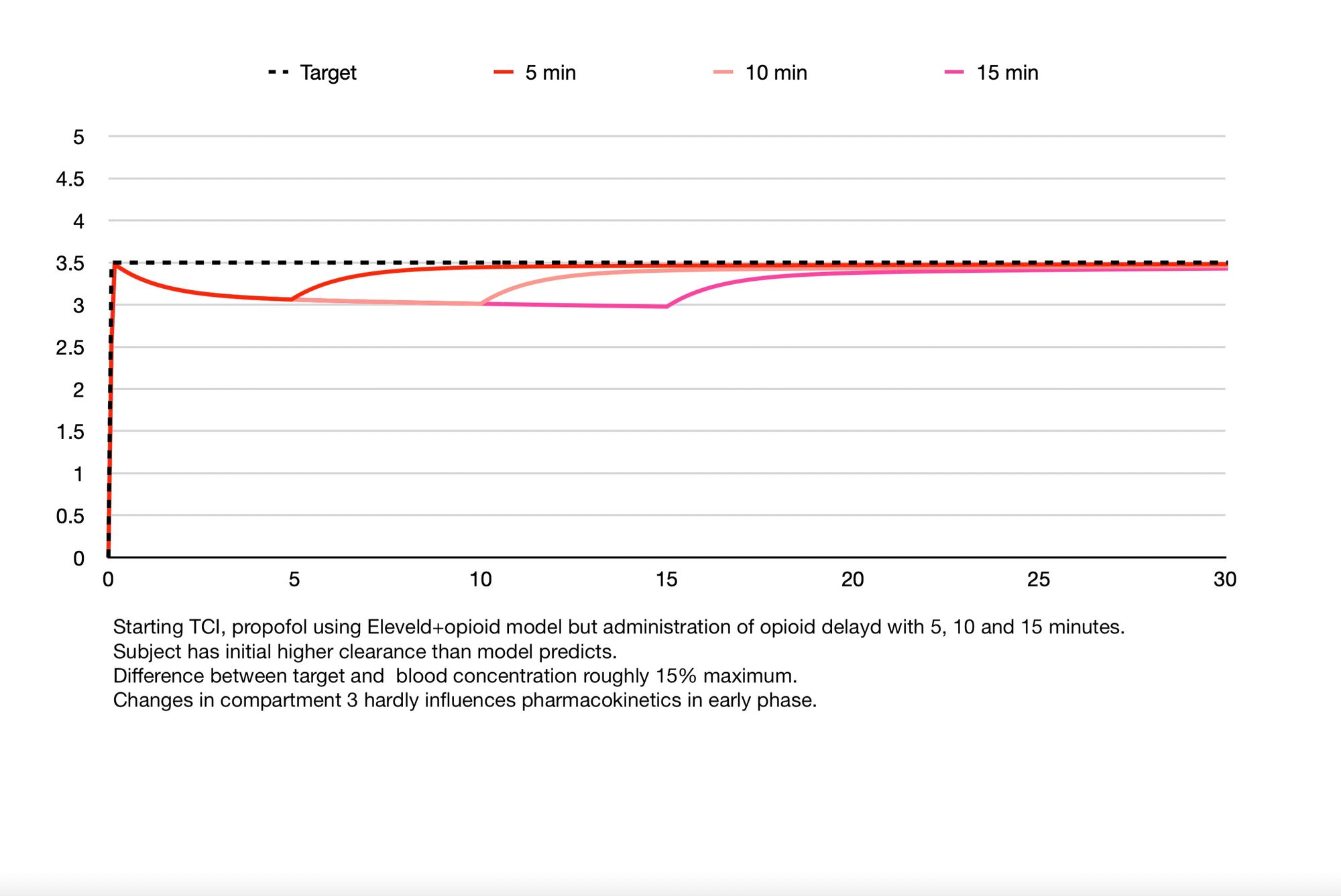
- You select Eleveld + opioid because opioid is intended to be given for incision but induction is without opioid. In the figure below this situation is simulated when the opioid is given 5, 10 and 15 minutes after induction. The simulation is achieved by setting the target to 3.5 µgr/ml in the TCI sheet[B] and selecting opioid (or setting True in excel) for all the timesteps[D]. Then copy the data in the pump rate column[G] and paste the results in the pump rate column of the induction sheet[F]. Make sure that you not simply paste the cells, but that you paste the results(numbers) or values(excel). Now you can select the period that no opioid was given by deselecting the cells in the opioid column[D]. Then copy the resulting concentrations as results(numbers) or values(excel) to a place in the spreadsheets where you can use them for graphing.
The following observations can be made:
- Because the central volume is not changed by the opioid the loading dose to achieve the target is the same with or without opioid. Thereafter the clearance of the patient(no opioid) is higher than predicted by the model(+opioid) therefore the concentration will drop roughly by 15%. the changes in the 3th compartment hardly play a role so early in the pk of the model.
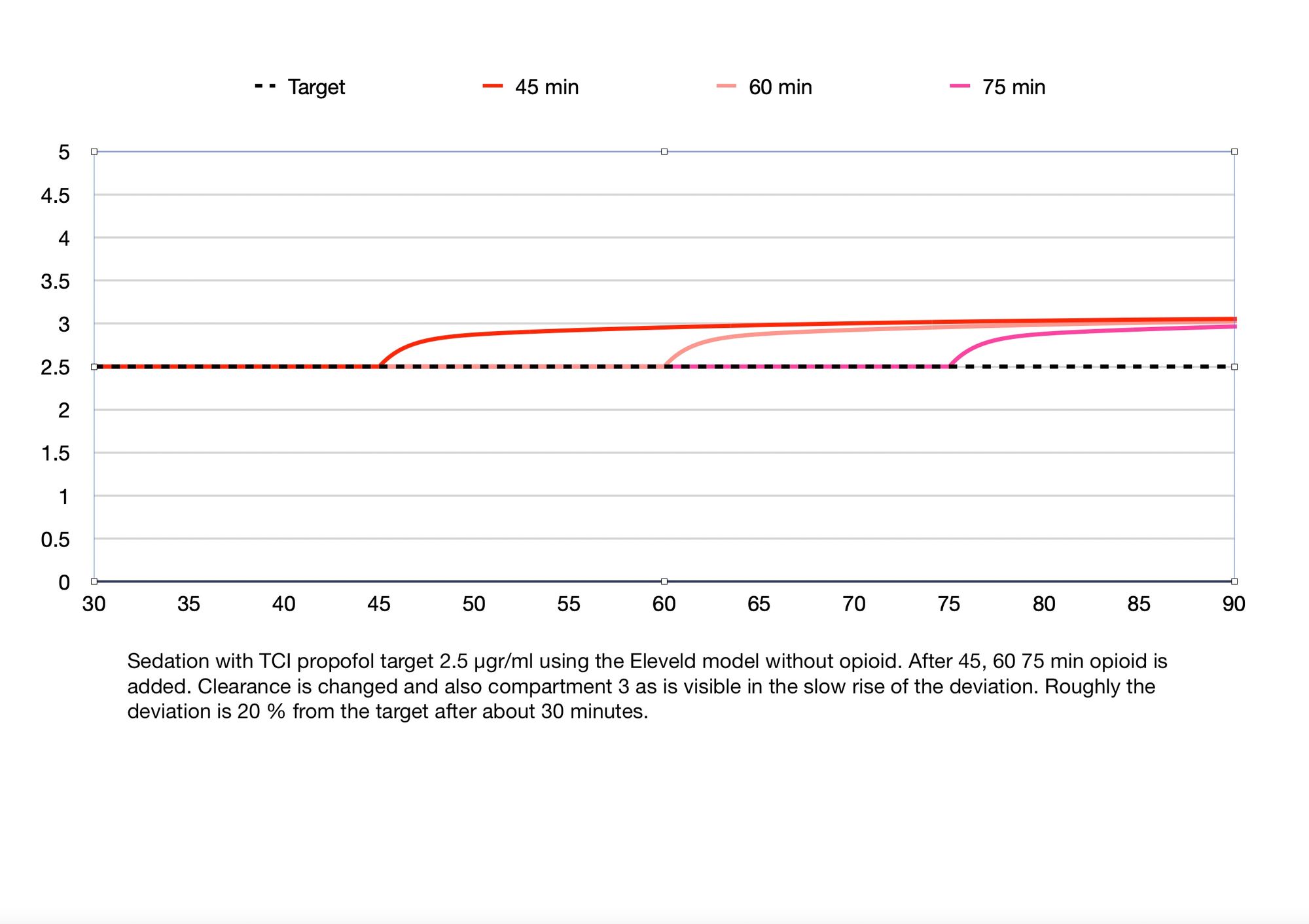
- You are performing a sedation with TCI, target 2.5 µg/ml, using the Eleveld model with no opioid. At a certain moment some opioid is needed to control a painfull stimulus for examle. In the spreadsheet a sheet is added called sedation for working with this scenario. Steps to perform are similar to the first scenario.
These simulations are obviously over-simplifications of real clinical scenarios. One of the limitations is that the opioid influence is not modelled dependent on the amount of opioid or potency of the opioid. Also they do not show the pharmacodynamic interaction of propofol and the various opioids. So adjustments of dosing solely based on these simulations is probably unwise. But they may help in understanding observations made in clinical practice and thereby help us with the task of titrating the anaesthetic drugs.
And still an aspect of the Eleveld paper is still untouched: The pharmacodynamics, involving the effect compartment, effect compartment control and the relation to the Bispectral Index. In the next blog I will use the spreadsheet appraoch to try to shine some light on these items.
For now: download the spreadsheets and play around with them and if you have questions, want to debate or add comments: use the form below the blog.